1. Introduction
ne of the major challenges facing our educational sector today is the infiltration of traditional beliefs into the schools system resulting in internal cognitive conflicts especially when the educational concepts violate traditional beliefs. Observations made during the supervision revealed that JHS 1 learners of a school in Assin Atonsu, a town that shares boundaries with Foso College of Education, show unacceptability of the concept of malaria taught in class because they have had proving pieces of evidence that people infected by malaria are healed by prayers and observing directives from herbal doctors so no amount of conviction with scientific evidence could make them agree to the causes and prevention of malaria. The purpose of this study was therefore to find out the causes and effects of learners' refusal to accept the concept of malaria taught in class and find appropriate strategies to investigate this misconception and right it.
In order to solve the problem of learners' gross exhibition of refusal to accept the concept of malaria taught in class, the study was guided by the following questions:
? What are the causes of JHS 1 learners' refusal to accept the concept of malaria taught in class? ? What are the possible strategies that could challenge this refusal among JHS 1 learners? ? To what extent can community walks and worksheets prove appropriate in eradicating this refusal among JHS 1 learners? It is the hope of the authors that the findings and recommendations in this study will equip basic school teachers with possibilities of outlining the misconceptions about academic concepts and ways of challenging them for their resultant academic progress to learners. It is obvious that any research work is bound to suffer hindrances and this research was no exception. Some of the difficulties encountered were; The subject for the study has minimum flirtations by authors and so coming by information for the study was a big blow. The study was also limited to action research which presented only pedagogic solutions. The findings of this research were also limited to descriptive analysis by the use of means, frequencies, tables and percentages.
2. II.
3. History of Malaria
Malaria, literally meaning "bad air" and formerly called ague or marsh fever due to its association with swamps and marshland, originates from the Mediaeval Italian word mala aria. Although the parasite responsible for malaria has been in existence for 50,000-100,000 years, until remarkable advances in agriculture and the development of human settlements, there was no increase in the population size of the parasite. (1). The "Roman fever" that was so pervasive in several regions in ancient Rome such as southern Italy, the island of Sardinia, the Pontine Marshes, the lower regions of coastal Etruria and the city of Rome along the Tiber (2) and causing the decline of the Roman Empire because of the favorable presence of stagnant water caused from Irrigated gardens, swamp-like grounds, run-off from agriculture, and drainage problems from road construction, preferred by mosquitoes for breeding grounds was later traced to be Malaria. (3) In Mediaeval West Africa, the people of Djenné successfully identified the mosquito as the vector and cause of malaria. (4) Around 1640, a drug, which happened to be the first effective treatment for malaria, was introduced in Europe by the Jesuits. This drug was extracted from the bark of cinchona tree, which grows on the slopes of the Andes, mainly in Peru whose indigenes made a tincture of cinchona to control fever and later found effective against malaria. By 1677, it was included in the London Pharmacopoeia as an antimalarial treatment. (5) It was in the 1820s that the active ingredient in the drug extracted from the bark, was isolated and named by the French chemists Pierre Joseph Pelletier and Joseph Bienaimé Caventou as quinine. (6) Quinine was the predominant malarial medication until the 1940s, when chloroquine replaced quinine as the treatment of both uncomplicated and severe malaria until resistance supervened, first in Southeast Asia and South America in the 1950s and then globally in the 1980s.
4. III.
5. Misconception about Malaria
According to (7) the general misconceptions about malaria include the following:
1. "I did not hear any mosquitoes so I won't be bitten.": The female anopheles mosquito is small and noiseless. She often doesn't leave a mark either. Many people believe that they don't get bitten by mosquitoes, especially if they don't hear them buzzing.
2. "I have had malaria, so I am immune.": The misconception regarding immunity and malaria puts many people travelling to malaria areas at risk. There are those who believe that once they have had malaria, they will be immune (similar to the measles situation) but this is not the case. Sleeping under impregnated bednets protects againts the anopheles bites during the night. The mosquitos have changed biting habits, their feeding time starts at dusk and ends at dawn, it is not correct as said at midnight. Drug prophylaxis has it sides effects yes, but the side effect of not taking it may be ending up at the grave yard. They do not give 100% protection, but they give us medical doctors time to give you effective treatment before the parasite kills you.
Stop spreading those lies, young unexperienced people may listen to you and end up seriuosly ill, life long handicapped with brain damage after cerebral malaria or die.
6. a) What are Field Trips?
Field trips, also known as instructional trips, school excursions, school journeys, are student experiences outside of the classroom at interactive locations designed for educational purposes through displaying and exhibiting to gain an experiential connection to the ideas, concepts, and subject matter. (9) (10)
7. b) Purposes of Field Trips
Field trips help to provide firsthand experience and stimulate interest and motivation in science by strengthening observation and perception skills (11). Also, learners have the opportunity to be taken to locations that are unique and cannot be modeled in the classroom but the connection between the field trip venue and the classroom links the field trip's experiential learning with prior experiences and learning from the classroom (12). apart from giving opportunity to encounter a multidimensional activity to learners in which all their senses are fully involved (13), they are also experiential, authentic social events that create a new way of knowing an object, concept, or operation (14). Quality experiences lead to deeper learning and interest development (13).
8. c) Kinds of Field Trips
Formal field trips consist of planned, wellorchestrated experiences where students follow a documented format. Teachers find such programs comfortable because the students are bound to a choreographed agenda. However, there are minimal opportunities for students to personally interact and connect to the experience (15).
Informal field trips on the other hand are less structured and offer students some control and choice concerning their activities or environment. Teachers are often amazed by how much students know and which students possess the most knowledge (15). Together, these qualities create an intrinsically motivated student (15) that encourages students to examine their connection to the local and national communities, as well as their connection to the local and global ecosystems (9). d) Barriers to Effective field Trips (11) identified seven barriers to successful field trips: 1. transportation; 2. teacher training and experience; 3. time issues such as school schedule and teacher's ability to prepare; 4. lack of school administrator support for field trips; 5. curriculum inflexibility; 6. poor student behavior and attitudes; and 7. lack of venue options.
Finding time for the trip and making arrangements for students who cannot make the trip adds tasks to an already busy teacher schedule (15,13). Teachers need to determine the logistics to transport students. Large introductory classes present unique challenges due to the need of larger transportation facilities, safety issues, more student logistical planning, and time lost trying to organize the large group (16). It is imperative that the teacher prepares the students for the field trip in order to maintain a level of control that will allow for learning to occur when the class arrives at the venue (18). (19) suggested that often, a teacher's biggest fear is losing control of the students once at the field trip location. Upon arrival at a field trip venue, students are often disoriented resulting in excited, explorative, and unrestrained behavior (20). The teacher should be prepared to focus the students' mental and physical energy towards participation at the venue (12).
9. e) The Role of the Teacher in Organizing Field Trips
Despite the educational benefits of field trips to learners, teachers are directly involved and participate in all the preparation and field trip activities to connect the school's science curriculum to the venue and its focus because the field trip should not be a stand-alone experience (24). The teacher visits the venue prior to the field trip to learn the layout and determine whether the venue is suitable for all the learners (22; 15). To satisfy the three variables that prepare students for field trips identified by (23) as understanding the venue layout, the focus of the activities, and being prepared to be in a "novelty space," the teacher should connect the students' experiences on the trip with concepts and lessons taught in the classroom. As the field trip begins, the teacher plays a role to make learners comfortable in the new environment by first communicating the venue's expectations to any unfocused or confused students (25). During the field trip, students experience learning in an authentic, informal, natural setting. Each student's prior knowledge, gained both from the classroom and from their personal out-of-school experiences, is used to make connections to the field trip experience (26). The teacher should keep the students engaged. Teachers often utilize worksheets to help students focus on exploring and learning the targeted concepts. Worksheets are quite effective when one worksheet is given to a small group, in which the students are better observers, interact more frequently, discuss the concepts, and ultimately develop more connections between the concepts and the experience (24; 15). Simple fill-in-the-blank task completion worksheets are not effective, when every student is responsible for his or her own data, where the focus is solely to fill in the data and not to explore or participate in activities (24). Finally, the teacher's actions after the field trip to reinforce learners accumulated experiences through discussion, activities, reading, a television show or movie should not be overlooked. (28; 24; 29; 30; 21). Students need to solidify their new ideas and observations which have not yet made connections. Reflection will help build those connections, as well as reinforce the successful connections already made on the trip. Students generate greater understanding as teachers develop potential connections through reflection (24). Students should discuss their observations and experiences, and in the case of elementary grades, create presentations to share with their classmates. During the remainder of the school year, the teacher should connect new classroom concepts to the students' field trip experiences (25). In Tal & Steiner's (21) examination of teacher's roles during field trips to museums, neither elementary nor secondary grade level teachers carried out quality postvisit activities. Teachers must recognize the importance of post field trip reflection and debriefing to maximize student interest and learning.
10. IV.
11. Methodology
The research design used for this study was an action research design. Action research design was chosen because the study focused on a specific problem in a particular setting, that is a JHS in Atonsu and because action research design helps the classroom teacher to establish conditions in the classroom which will enable him/her achieve a particular result. The purposive sampling and census techniques were used to involve all twenty-eight JHS 1 pupils both boys and girls. These sampling techniques were used because they provided the opportunity for all the pupils to be engaged in the intervention processes since all of them showed gross refusal to accept the concept of malaria taught in class. The research instruments used were test items and observation. Observation was carried out during the teaching of malaria in class. It was observed that as the student-teacher was explaining the causes of malaria, the pupils continually shook their heads in disagreement because they had already been saturated in the traditional beliefs of malaria transmission.
The authors used test items for the pre and post intervention analysis. These were recorded and used to establish the fact that these were real problems at the pre-intervention stage and to see the effectiveness or otherwise of the intervention put in place at the postintervention stage.
12. a) Pre-Intervention Data Collection
Immediately the student-teacher finished facilitating a lesson on the causes and prevention of malaria, the authors conducted pre-intervention test to find out the pupils' understanding on the topic. The test was made up of eight supply type questions on worksheets, adapted from a WHO document. After the marking, it was observed that the performance was not encouraging.
Pupil Name: __________________________________ Instructions: Answer all the questions in this assignment. When you complete them all mail the assignment or bring it in person to AMREF.
13. b) Intervention Process
The authors met the head teacher to get him informed about the need to take pupils on a community walk to enhance their understanding on the concept of malaria. Then the authors discussed with them that they were about embarking on a community walk to the College of Education, the two Nursing and Midwifery Colleges, the Hospital, the river banks and part of Atonsu town behind the river. The head teacher in turn stamped the letters to the principals of the various institutions assembly man and chief of Atonsu. The essence of the community walk to these places was to allow the learners have a feel of a new environment outside the classroom for learning in a relax atmosphere and to observe how health and teacher trainees were seriously taken through the concept of malaria and how a complete ward is reserved for malaria patients to receive intensive care.
14. c) Intervention Design and Implementation Week 1 day 1: Objectives:
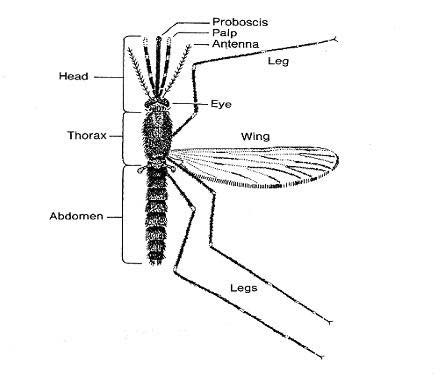
By the end of the session, every pupil should be able to 1. Examine the female anopheles mosquito and discuss its parts Discuss the breeding grounds for mosquitoes
15. Procedure:
A picture of a labeled female anopheles mosquito was projected for the pupils to observe and discuss what they thought the various parts were used for. Students talked about using the wings to fly, the eye to see. The nose to smell, the proboscis to suck etc. a detailed discussion about the mosquito was done and after the pupils were prepared for the excursion.
16. Activity 2
The authors went with her pupils to Assinman Nursing and Midwifery Training College where one student nurse guided on the tour. The authors and her pupils discovered that there was a choked gutter just in front of the entrance of the gate which could serve as a breeding ground for mosquitoes. Pupils were given a magnified lens to view the larvae of mosquitoes. At the back the college is a swampy area which could also serve as a breeding ground. The second place visited was the Foso College of Education. They were led by a Science tutor who served as a resource person for the tour. The resource person took the pupils around and showed them their drainage system. It was noticed that all their water passes through covered gutters and for that matter it cannot serve as a breeding grounds for mosquitoes. The resource person however took them to a swampy area on campus. This was a place where the soil texture had a capacity to retain water for a long time so as it rained, the water became stagnant there, as he made a sweep with his hand over the stagnant water, the pupils could see mosquitoes flying about. Again at the entrance opposite the supermarket is a refuse dump where mosquitoes were also seen in empty open cans and other containers that could hold water. The pupils had the opportunity to visit the outskirts of the ladies' dormitories where buckets of water were kept. It was noticed that some mosquitoes had already found these as safe places to breed. The tutor brought us back to campus and showed us the numerous garbage bins with tight lids placed at vantage points on campus. These and the covered gutters, he said were measures of preventing mosquitoes from breeding.
When we returned to school, a recap of the visit was done with pupils and the following worksheets were given them in groups to fill and present. A long proboscis (the adapted mouth parts), which projects forward and which the female uses to pierce the skin when taking a blood meal; A body and wings covered with scales; and Wings with veins which show a definite pattern There are over 2,600 known species of mosquitoes in the world. However, in Africa we are mainly concerned with two species namely, the An gambiae sl and An funestus. The life cycle of a mosquito has four distinct stages of development, egg, larvae, pupa and adult. The eggs, larvae and pupae stages are aquatic but the emerging adults are free-flying insects. Mating usually takes place immediately after the adults emerge from the pupa before females seek a blood meal. Both females and males suck nectar and other plant juices as energy sources; but females require a blood meal for maturation of eggs. Mosquitoes rest either indoor or outdoor during the day in cool humid locations to minimize moisture loss. Their biting activities take place from dusk, throughout the night until just before dawn, feeding either indoor or outdoor. Mosquitoes have preference for various hosts (Human & animal) for their blood meal; however, efficient malaria vectors have preference for human blood.
17. Week 1 day 2 Objectives
By the end of this unit you should be able to: Define malaria Write down the importance of malaria
Examine the malaria parasite.
18. Procedure
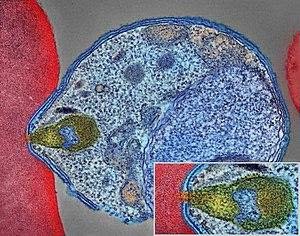
The authors, with the help of a community voice had a whole class discussion on malaria with the pupils. The community voice took the pupils through the following As we begin our discussion, it is important for us to know what Malaria is and its importance Malaria is a febrile disease caused by the blood parasite called Plasmodium transmitted by the bite of an infected female anopheles mosquito. Malaria is the most common disease in Africa. It is also the number one cause of death among young children and a significant cause of miscarriages among pregnant mothers. About 95% of children brought to health facilities with fever suffer from Malaria. A significant amount of suffering, complications and death due to malaria can be prevented through prompt and correct treatment and prevention measures. After, the authors had a discussion on the importance and impact of malaria on the society with the pupils. Then a picture of the malaria parasite was projected for the learners to see.
Describe the life cycle of the malaria parasite ??????????????????????????? ??????????????????????????? ??????????????????????????? ??????????????????????????? Now compare your answers with the following discussion.
? The public health importance of malaria One-fifth of the world's population is at risk of malaria. According to WHO there are between 300 -400 million cases of malaria illness annually (WHO1).
The greatest burden and most deaths occur among African children and are on the increase. It endangers the health of women and newborns.
Malaria epidemics cause high morbidity and mortality in areas where they are prone particularly in the highland areas.
There has been progressive spread of malaria into areas which had been free of the disease in the recent past.
Malaria is therefore, an important disease requiring special attention.
? The public health impact of malaria 1. The disease causes widespread premature death and suffering 2. Imposes financial hardship on poor households, 3. Holds back economic growth and improvements in living standards. 4. Acute febrile illness, chronic debilitation, complication of pregnancy, and impairment of the physical development and learning ability of children.
19. Time lost and physical inability to engage in
productive work and contribution to economic welfare translates directly into economic loss and impacts negatively in the quality of life of individuals, their dependence and or caretakers incase of children.
20. Costs to individuals and their families include:
purchase of drugs for treating malaria at home; expenses for travel to, and from health clinics; lost days of work; absence from school; expenses for preventive measures; expenses for burial in case of death and other incidental expenditures. 7. Costs to governments include: maintenance of health facilities; purchase of drugs and supplies; public health interventions against malaria, such as insecticide-treated nets; lost days of work with resulting loss of earning; and lost opportunities for joint economic ventures. Such costs can add substantially to the economic burden of malaria particularly in endemic countries and strongly impedes their economic growth.
21. Week 1 day 3 Objectives
By the end of the lesson, every learner should be able to Differentiate an Anopheles mosquito from the other mosquitoes Describe the life cycle of both the anopheles mosquito and the culicine mosquito.
22. Procedure
Because of the prior arrangement made with management of the college of education for the visit, this day walk was an enjoyable one. The time was 7:00 a.m. We arrived there to join the science students in their study of the differences between the anopheles mosquito and others and their life cycles. Before the start of the session, all of us were made to go round the premises and identify mosquito prone areas. Equipment was given us to attract as many mosquitoes as we could. When we came back, lenses were given us to observe the types of mosquitoes caught. The images of both mosquitoes were projected for pupils to observe.
After the lesson, the facilitator met us for questions and clarifications. When the leaqrners admitted that they had understood everything, we were granted leave and came back to school. Each learner was given a worksheet to fill out the differences observed between the anopheles and other mosquitoes. Then a whole class discussion was held.
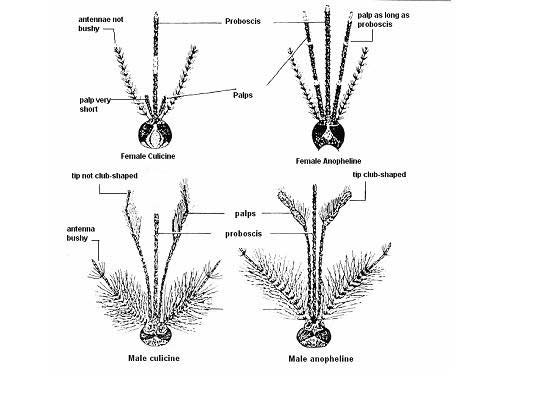
23. Some distinguishing features of Anopheline and Culicine mosquitoes
How well can you differentiate an Anopheles mosquito from other Mosquitoes? i. Female anopheline????????????????????????? ii. Culicine ?????????????????????????? iii. Male anopheline???????????????????????? iv. Culicine ?????????????????????????? One way that anopheline mosquitoes can be distinguished from culicines is by the length and shape of the palps.
Female anophelines have palps as long as the proboscis Female culicines have palps which are much shorter than the proboscis Males Anophelines have palps longer than proboscis and are club-shaped at tip Culicine have palps longer than proboscis, with tapered tips.
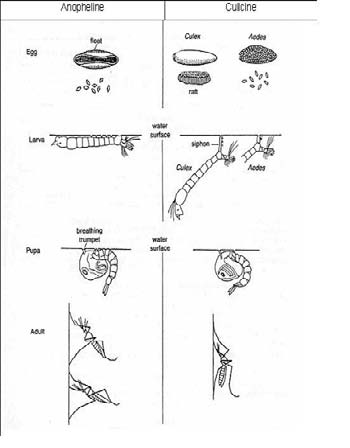
Then the life cycle of the two mosquitoes were projected and discussed as follows
24. Life cycle of anopheline and culicine mosquitoes
Another way of distinguishing anopheline and culicine mosquitoes is by observing the following: Culex eggs clump together forming a "raft". Aedes eggs float singly, Anopheles eggs have floats.
The anopheles larvae rest parallel to the water surface, breathing with specialized hair at last segment. This is in contrast with culicine larvae which rest at an angle to the water surface and has a long siphon for breathing. The pupae for both species are active and do not feed.
The adult anopheles rests at an angle while culicine rests parallel to the resting surface respectively.
25. Week 2 Day 1
This day's excursion was done at Nursing School 1. Because the purpose of the visit was already known to the authorities, the principal of the school invited us to the lecture theatre where the students were all set for lectures. The topic was the specie of the plasmodium. The learners observed how seriously the nursing students had taken the lesson. This was a way of challenging their misconception that if malaria was indeed a spiritual disease, why would both teacher and nursing training institutions spend time studying it in formal educational set ups.
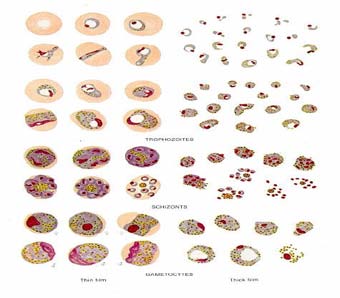
Back at school, the authors modified what the nursing students studied in simple language with the help of the following WHO document. Plate 1 Appearance of Plasmodium falciparum stages in Giemsa stained thin and thick blood films Plate 2 Appearance of plasmodium malariae stages in Giemsa stained thin and thick blood films Plate 3 Appearance of plasmodium ovale stages in Giemsa stained thin and thick blood films.
The four species of Plasmodium which are known to cause disease in man are:
26. Plasmodium vivax (Tertian).
It is the most common species in the World. It is the largest of the malaria parasites found in humans. The length of its asexual cycle is 48 hours. Relapses are common in vivax malaria due to emergence of new blood forms from maturing secondary liver schizonts. In tropical areas, relapses may arise within three to four months of primary attack, while in subtropical areas relapses occur only after nine months or more.
27. Plasmodium ovale, (Tertian)
It is a relatively a rare species with a frequency of less than 5%. It may sometimes be confused with P. vivax. The length of its asexual cycle is 48 hours. Relapses occur as in P. vivax but the disease tends to be more chronic.
28. Plasmodium malariae. (Quartan)
It is a less common species whose length of its asexual cycle is 72 hours. P. malariae is associated with quartan malaria.
29. Plasmodium falciparum, (Sub-Tertian)
It is the commonest species in Africa and it accounts for 95 -98% of all malaria infections. It is responsible for severe illness cerebral malaria and other complications and may cause death. The length of asexual cycle is about 48 hours. Fever is produced when the schizonts are mature i.e. at 48 hours interval. Sub-tertian means that diurnal periodicity is common. The liver stage of development take about 14 days.
In our environment, you may have noticed that many malaria laboratory tests report the presence of P. falciparum. This is because it is the most common cause of malaria in our environment. Indeed in Africa, Plasmodium falciparum is the most common type of malaria parasite transmitted in Africa, south of the Sahara, accounting in large part for the extremely high mortality in this region.
Back to school the worksheets were given the pupils to work on as assignments.
List down the four (4) species of Plasmodium
i) ???????????????????????????? ii) ????????????????????????????? iii) ???????????????????????????? iv) ????????????????????????????? Outline one characteristics of each species i) ?????????????????????????????? ii) ?????????????????????????????? iii) ????????????????????????????? iv) ??????????????????????????????30. Week 2 Day 2 Objectives
By the end of the lesson, every learner should be able to discuss the life cycle of a mosquito. This day's facilitation was done in the learners' own class for the purposes of addressing any future misconceptions that issues about malaria were to be studied in higher institutions. The facilitation was designed as a progression of what the two institutions had studied.
The different biting styles of mosquitoes were projected for pupils to observe.
Then the following discussion proceeded.
As we mentioned earlier, malaria is transmitted by the female Anopheles mosquito which requires blood for the development of its eggs. These eggs are laid on stagnant water or slow flowing water where they stay for 2-3 days before they hatch to release mosquito larvae. The larvae grow beneath the water surface and become pupa. After a few days the pupa develops into adult mosquitoes and flies away. The development of mosquitoes from egg to larvae to adults takes 7-14 days at a temperature of 31oC or 20 days at 20oC. If the adult mosquito is female, it looks for a blood meal to facilitate egg development, thereby starting the development cycle all over again. If the adult mosquito is male it feeds on plant juices. When a mosquito sucks the blood of a person who has malaria parasites in his or her blood, the mosquito picks male and female gametocytes where they undergo a series of changes to become sporozoites. The sporozoites are the infective stages of malaria parasites in the mosquito. This process called sporogonic cycle takes about 10 -14 days depending on environmental temperature. When a mosquito carrying sporozoites bites a person, it passes the parasites into The Malaria Life Cycle By the end of the lesson, every learner should be able to mention three vectors involved in malaria transmission.
31. Procedure
On this day, because it was assumed that the pupils knew something about malaria transmission, the worksheets were given to them before the start of the lectures.
32. Mode of Transmission of Malaria:
Before you read on, here is an activity to enhance your learning process, take about 10 minutes to think about it and write out your answer.
How is Malaria transmitted? Name the vector involved in the transmission. ????????????????????????????????? ????????????????????????????????? ????????????????????????????????? ????????????????????????????????? ????????????????????????????????? Then the following note was projected on the screen for pupils to read at random. As pupils read paragraph by paragraph, the facilitator describes the process on the projected diagram. The Malaria parasite lifecycle begins when an infected adult female Anopheles mosquito bites a human being to feed on his or her blood. As it feeds on this blood, it releases malaria sporozoites (parasites) into the blood stream of the host (human being). This is the infective bite. Once the parasites enter the human blood stream they move quickly to the liver cells where they develop and multiply (schizogony). The infected liver cells rapture and release numerous merozoites into the blood, which invade red blood cells (RBCs). This stage takes 9-14 days. Within the RBCs the parasites develop from "rings" into blood schizonts. The schizonts then rupture the RBCs releasing numerous merozoites which invade new RBCs. When the infected red blood cells rapture, this process initiates the chills and fever which are characteristic of Malaria. Indeed, the peaks of fever experienced during malaria coincide with the release into blood circulation of malaria parasites (merozoites) from raptured RBCs.
The period between the infective bite and the onset of symptoms (i.e fever, chills etc,) is called the incubation period of malaria. As we mentioned earlier, the incubation period is usually 7-14 days but may be shorter as in P. falciparum or longer in the case of P. vivax and P. malariae. See figure 5 for an illustration of the cycle of malaria.
There was a discussion on the transmission. As the facilitator explained, he points to the stages on the diagram projected alongside.
In the space provided below and in your own words; describe the life cycle of the Malaria parasite. ????????????????????????????? ????????????????????????????? ?????????????????????????????
33. Week 3 Day 1
On week three day 1 the learners were asked to give two reasons why we should promptly treat malaria at each of these stages. After the whole class discussion, the following points were established on the two stages of malaria.
Uncomplicated Malaria: It presents with fever, chills, nausea, vomiting, headache, joint pains, general malaise, and profuse sweating. It is important to promptly diagnose and treat uncomplicated malaria for two reasons:
To avoid the disease progressing to a severe and complicated situation
To reduce the number of parasite carriers within the community and hence interrupt further transmission
34. Severe Malaria:
This is a form of life threatening malaria that can affect many systems of the body as shown in the following table.
Malaria complications are life threatening so we should stop the clinical stage from progressing by early diagnosis and administration of the correct treatment. After the short discussion that served as an introduction to malaria, the visit to the hospital was a perfect compliment. The official in wait for us welcomed us and led us to the conference room where the medical practitioners were having a PDS. The doctors discussed the signs and symptoms of malaria and prepared to visit the malaria ward to see how the patients showed different signs and symptoms. There were some receiving infusions, others given transfusion, nurses administering drugs to others and some throwing up. Some temperatures read 38 0, and other patients shivering with cold. We were made to observe the conditions of those with uncomplicated malaria and those with severe malaria. The differences were obvious. Those with mild attacks could speak, move around and eat but almost all with severe malaria were either on infusion or transfusion because of extreme weakness and blood shortage respectively and others being managed at critical points. This visit had a positive effect on the learners because as the facilitator explained, if it were a spiritual disease, the various tests run on them would not have shown the presence of the parasite and patients would not have responded to treatment. He also addressed that no matter how insignificant the plasmodium parasite may look, once they attack the blood of their host and the blood circulates, it carries the parasites along and very soon the whole blood is infected that is why malaria remains the fastest killer disease if not diagnosed and treated early.
35. Week 3 day 2
By the end of the lesson, every pupil will be able to 1. List three activities of indigenes that promote malaria infection 2. Educate the indigenes of ways of preventing malaria infections. 3. Initiate communal labour to clear all weedy places in and around the school premises. Beside these educational visits, there was a visit to the Atonsu River. People around the river have poor drainage system. It was noticed that they poured dirty water anywhere and anyhow because they believe that it will drain to the river. These dirty water thrown around anyhow served as breeding grounds for mosquitoes since some are stagnant.
From there, the authors with the pupils went to the river banks and realized that there were dense forest canopy around each side of banks and hence serve as a hiding place and breeding ground for mosquitoes.
The next activity was to educate the people around the bank of the river. Pupils were put in pairs to visit households and educate them on the causes and symptoms of malaria as well as its prevention. The pupils were prepared for this through the discussion of problem solving and cultural identification skills.
The learners were poised for action. The time for communal labour which was fixed at 4:30 p.m was scheduled with the people. It was a successful campaign.
At exactly 4:00 p.m. the learners had started gathering with their weeding tools. At 4:30 p.m. we marched to the areas earmarked for the activity: in and around the school premises, the banks of the river and the community center. It was surprising how members of the community joined hands to complete this malaria eradication activity.
36. Week 3 day 3: Post -Intervention
By the end of the lesson, every learner should be able to demonstrate independent learning skill by answering the following questions.
You have now come to the end the intervention session. For the past three weeks, we have managed to define malaria, discussed its causative organism, its life cycle and mode of transmission. If you have are satisfied that we have achieved the learning outcomes, do the attached assignments for marking. If you have any problems in understanding any of the sections, do not hesitate to consult me about it.
Pupil Name: __________________________________ Instructions: Answer all the questions in this assignment. When you complete them all mail the assignment or bring it in person to AMREF.
37. i. The Causes of Pupils' Refusal to Accept the Concept of Malaria Taught in Class
Table 1 discusses the causes of pupils' refusal to accept the concept of malaria. A poll was taken for pupils to write down why they did not accept the concept of malaria taught in class. It could be seen that out of the 28 pupils, 4 representing 14% said that they had not experienced the disease before so they couldn't imagine what the teacher was talking about. They said they had never contracted it nor seen anybody have it so the concept was abstract to them. 15 pupils representing 54% chose traditional beliefs. They said ever since childhood, they have been made to believe that Malaria is only contracted if demons make one their target and infect them with it. According to them, it is only a strong and powerful man of god who can, through prayers and pacifications heal an infected person of the disease. Unscientific healing procedure was also chosen by 3 pupils who said per their own experience, it took the drinking of concoctions and other traditional processes like subjecting one in a very hot water temperature and batheing with salty water. No other methods would prove efficacious apart from what they had really trusted. Lastly, teachers' poor method of teaching attracted 6 pupils constituting 21% because the pupils said the teachers only talk without illustrations and any touch to practicality. Because majority of the learners admitted that because of their traditional beliefs about the spread of malaria, it was difficult accepting what the teacher was saying, the authors probed further to know the which beliefs militated against the scientifically proven information about malaria taught in class. The learners were told to list two of the beliefs they know about the causes and prevention of malaria. From table 2, it can be concluded that 24 of the learners, forming 86% said that malaria is a spiritual disease. They never understood why a tiny creature like mosquito can cause malaria. They questioned, 'how huge and strong is the mosquito to contain such a parasite which can kill humans?' Again 16 learners felt that only spiritual men could cure malaria by pacifying the spirit beings responsible for its transmission. They believed that being prayed for and given spiritual directives will keep these spirit beings away to complicate the disease so that the concoctions prepared for you could heal you. 26 other learners constituting 93% posited that all the orthodox medicines available were manufactured from herbs so if there is the need to full potency of a drug, the herbal product should be more preferable to the orthodox ones which had gone through some artificial processes to reduce its efficacy. The strategies to challenge the misconceptions pupils have malaria was discussed with pupils. The items were explained and the pupils were tasked to choose one. Work sheets was chosen by 6 pupils representing 21%. They said since that will give them some practical touch to the lesson, they would very much want to work with it. Video shows pulled down 7 pupils representing 25%. They posited that something they could not imagine will best be close to real when shown on videos. All their senses would be activated to feel, hear, see, what it means to be infected by malaria. A resource person's visit was equally attracted to 5 pupils representing 18%. They felt that perhaps if an expert in the field handled the concept, it would be more interesting, more information packed and more activity based. However, community walk swept away 10 pupils representing 36%. They said they wanted to visit places where they could a feel of the real situation. Getting to know places where mosquitoes breed, the causes of malaria, symptoms and prevention and seeing people who are receiving treatment other than what they have been exposed to, will go a long way to satisfy their curiosity for a better understanding of the concept. From table 3, it could be realized that the preintervention test results was nothing good to write home about as compared to the post-intervention test results while 16 pupils representing 58% scored between 0-5 in the pre-intervention test, only 3 pupils representing 11% scored it during the post intervention. A percentage drop of 47% is a remarkable achievement to note. Again score 6-10 attracted 6 learners representing 21% at the pre-intervention but at the post intervention 2 pupils representing 7% scored it. Here too a 14% decrease was realized. This showed that the range from fail to average recorded a 61% drop signifying an improvement in performance was realized with a conclusion that the concept was now becoming understandable to pupils. Score range of 11-15 attracted 2 pupils constituting 7% while at the postintervention test, 7 pupils representing 25% scored it. In the same achievement trend, score 16-20 attracted 4 pupils representing 14% at the pre-intervention test while a huge number of 16 pupils representing 57% scored it at the post-intervention test. A percentage rise of 61 % was acknowledging enough to call for a celebration.
38. Summary of the Study
The main objective of the study was to examine the causes of pupils refusal to accept the concept of malaria among JHS 1 learners of Census and purposive sampling procedure were used to select all twenty-eight pupils for the study. The sample is made up of 16 boys representing 12 girls representing. The data were presented using descriptive statistics.
The study identified the following as major findings.
1. Causes of refusal to accept the concept of malaria among JHS1 pupils comprise never experiencing the disease, traditional beliefs, unscientific healing procedures, teachers' poor teaching methods. VII.
39. Conclusion
The findings showed that never experiencing the disease, traditional beliefs, unscientific healing procedures, teachers' poor teaching methods are the causes of the inability of pupils to understand the concept of malaria among JHS 1 learners as shown in the literature review.
The views of the pupils led to the conclusion that work sheets, video shows, resource person's visit, community walk, was considered to be the most important strategy to reduce inability of pupils to understand the concept of malaria among JHS 1 learners.
40. VIII.
41. Recommendations
Based on the findings and conclusions of the study, the following recommendations are made.


| Also, | (8) | documents | the | following | |
| misconceptions about malaria. | |||||
| 1) These | |||||
| days tonic water hardly contains quinine, and you'd | |||||
| have to drink some 150 litres per day -even if you'd | |||||
| manage this, I suggest you do not mix it with gin. | |||||
| 2) I keep mosquitoes at bay with ultrasonic devices. | |||||
| This nonsense persists simply because from time to | |||||
| time industry tries to fool us into buying such | |||||
| gadgets. They supposedly produce high-frequency | |||||
| male mosquito sounds that would keep the female | |||||
| away from you. Not so. In fact, selling such gadgets | |||||
| ought to be viewed as unethical. | |||||
| 3) I eat lots of garlic and drink my beer. Numerous | |||||
| stories about food sources that reduce your | |||||
| attractiveness to mosquitoes persist. Fact is that | |||||
| there is hardly any evidence that garlic and Vitamin | |||||
| 5) I stay in luxurious hygienic places. Hungry female | |||||
| mosquitoes ignore the price you've paid for your | |||||
| accommodation. Although luxurious places often do | |||||
| better in terms of keeping mosquitoes out | |||||
| (screening, bednets), once you sit on your veranda | |||||
| at night you'll be on the mosquito menu. | |||||
| 6) There is no malaria-risk in urban centres. Even this | |||||
| doesn't hold. Many large urban centres that you will spend a night or two in before and after your safari have malaria. Though most cities were free of malaria during colonial days because of laws banning intra-urban agricultural practices, such activities have returned and are providing superb breeding sites for mosquitoes. 7) My partner always gets bitten so I don't need to worry. It is indeed true that, given a choice, female malaria mosquitoes will preferentially select one of | vivax could stay in your liver for a long time, we could eradicate them. 10. "If you take an antimalarial tablet, you can be sure that you will not get malaria.": No antimalarial medication is 100% effective when used to prevent malaria. Most of them are around 80-95% effective, that means you could get malaria while you're taking antimalarial medication. And in this situation, | ||||
| you. If you're the lucky one, don't count yourself rich | |||||
| -if your partner is not around you will still be bitten | |||||
| and run the risk of contracting disease. | |||||
| Causes | Frequency | Percentage |
| Never experiencing the disease | 4 | 14 |
| Traditional beliefs | 15 | 54 |
| Unscientific healing procedures, | 3 | 11 |
| Teachers' poor teaching | 6 | 21 |
| Total | 28 | 100 |
| Strategies | Frequency | Percentage |
| Work Sheets | 6 | 21 |
| Video Show | 7 | 25 |
| Resource Person's Visit, | 5 | 18 |
| Community Walk | 10 | 36 |
| Total | 28 | 100 |
| Year 2021 | |||||
| 56 | |||||
| Volume XXI Issue XV Version I | |||||
| G ) | |||||
| ( | |||||
| -Global Journal of Human Social Science | Class Marks 0-5 6-10 11-15 16-20 Total | Pre-test 16 6 2 4 28 | (%) 58 21 14 100 7 | Post test 3 2 16 28 7 | (%) 11 7 25 57 100 |
| © 2021 Global Journals |